Blood Biomarkers for Rare Neurological Diseases
A Comprehensive Guide for 2026
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Introduction
Rare neurological diseases collectively affect millions of patients worldwide, yet each individual condition may strike fewer than 1 in 2,000 people. For decades, clinicians faced a frustrating reality: the brain hides behind the blood-brain barrier (BBB), and meaningful biomarkers required invasive cerebrospinal fluid (CSF) sampling, expensive imaging, or post-mortem confirmation. The advent of ultra-sensitive blood-based biomarker assays is rewriting that playbook. Today, a simple venipuncture can reveal axonal injury, astrocyte stress, protein misfolding, and even target engagement of brain-penetrant therapeutics.
This article surveys the rapidly evolving landscape of blood biomarkers for rare neurological diseases — the biology that makes them possible, the technologies that detect them, the conditions they serve, and the clinical and research questions they answer.
Why Blood Biomarkers Matter in Rare Neurology
Rare neurological diseases — including spinal muscular atrophy (SMA), Huntington’s disease, amyotrophic lateral sclerosis (ALS), Friedreich’s ataxia, leukodystrophies, lysosomal storage disorders, and prion diseases — share several diagnostic challenges:
- Long diagnostic odysseys. Patients often wait 5–7 years before receiving an accurate diagnosis.
- Heterogeneous progression. Even within a single mutation, age of onset and disease course vary widely.
- Limited objective endpoints. Clinical scales are subjective and insensitive to early change.
- High therapeutic stakes. Gene therapies, antisense oligonucleotides (ASOs), and small molecules are expensive and demand objective evidence of target engagement.
Blood biomarkers address all four challenges. They support earlier diagnosis, stratify risk, track progression, and demonstrate pharmacodynamic effects. Critically, blood is accessible, longitudinal, and scalable — properties that CSF and imaging cannot match. For ultra-rare diseases scattered across geographies, blood-based assays also enable decentralized trials and remote monitoring.
The Brain-to-Blood Journey
Before discussing specific biomarkers, it helps to understand how brain-derived molecules reach the bloodstream. Three principal routes are recognized:
- Glymphatic and meningeal lymphatic drainage. Bulk CSF flow exits the cranium into cervical lymphatics, where solutes equilibrate with venous blood.
- Direct BBB transit. Smaller proteins (e.g., neurofilament fragments) cross a permeable or compromised BBB.
- Extracellular vesicle (EV) release. Neurons, astrocytes, and oligodendrocytes secrete exosomes and microvesicles that traffic into peripheral circulation, carrying intracellular cargo (proteins, RNAs, lipids) protected by a lipid bilayer.
Each pathway has practical consequences. Diffusible proteins reach blood roughly in proportion to brain damage; vesicle-encapsulated cargoes preserve cell-of-origin information and can be enriched by immunocapture — opening windows onto neuron-specific intracellular biology.
Major Classes of Blood Biomarkers
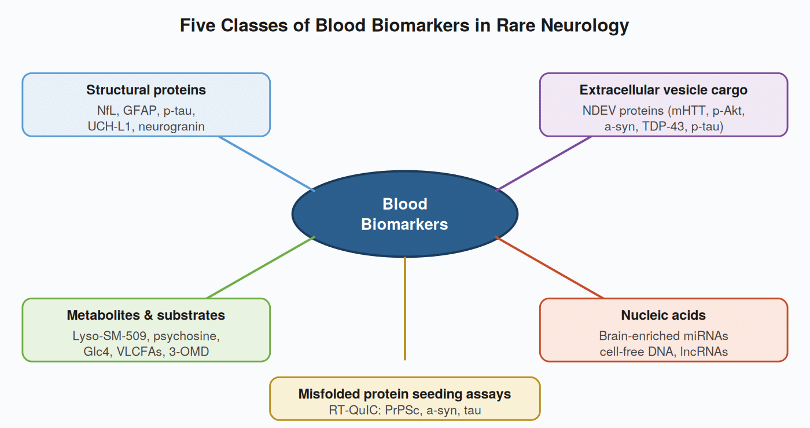
1. Neurofilament Light Chain (NfL)
Neurofilaments are intermediate filaments of large-caliber myelinated axons. When axons degenerate — regardless of cause — NfL is released into interstitial fluid, CSF, and blood. The Single Molecule Array (Simoa) platform enabled the first reliable serum and plasma NfL assays, with sensitivity in the low picogram range [1,2].
NfL has become a near-universal axonal injury marker. In rare neurological diseases, documented utility includes:
- SMA — plasma NfL declines rapidly after nusinersen, onasemnogene abeparvovec, or risdiplam initiation, particularly in infants [5].
- ALS — higher baseline NfL predicts faster progression; the FDA accepted NfL as a supportive biomarker in tofersen’s accelerated approval for SOD1-ALS [6].
- Huntington’s disease — NfL rises in premanifest mutation carriers years before motor symptoms and tracks with caudate atrophy [4].
- Friedreich’s ataxia — NfL distinguishes patients from controls and correlates with severity.
- Atypical parkinsonisms (MSA, PSP) — NfL helps differentiate these from idiopathic Parkinson’s disease.
2. Glial Fibrillary Acidic Protein (GFAP)
GFAP is the principal intermediate filament of astrocytes. Plasma GFAP rises in astrogliosis and astrocyte injury. Most studied in Alzheimer’s disease and traumatic brain injury (where it has FDA-cleared clinical use), GFAP is now relevant in:
- Alexander disease, a leukodystrophy caused by GFAP
- Adrenoleukodystrophy and other leukodystrophies with prominent astrocytic involvement.
- Antibody-mediated CNS disorders with astrocytopathy (e.g., AQP4-IgG NMO).
- Frontotemporal dementia with progranulin mutations [7].
3. Phosphorylated Tau (p-tau)
P-tau181, p-tau217, and p-tau231 have revolutionized Alzheimer’s diagnostics [8]. For rare disease, tau has more focused applications — notably in primary tauopathies (frontotemporal dementia subtypes, progressive supranuclear palsy, corticobasal degeneration), where total and phospho-tau ratios are under active investigation [13]. Plasma total tau is also markedly elevated in sporadic Creutzfeldt-Jakob disease and aids differential diagnosis.
4. Neuronal-Derived Extracellular Vesicles (NDEVs)
Perhaps the most exciting recent advance is the ability to immunocapture brain-cell-derived exosomes from peripheral blood [9]. Antibodies against neuron-enriched surface markers allow enrichment of vesicles whose interior cargo reflects intracellular brain-cell biology — a signal otherwise lost when measuring bulk plasma proteins.
NDEV cargo studied in rare neurological diseases includes:
- Mutant huntingtin protein in Huntington’s disease.
- Phosphorylated alpha-synuclein in synucleinopathies.
- TDP-43 species in ALS and frontotemporal dementia.
- Phosphorylated and total tau across tauopathies.
- Phosphoproteins reporting kinase pathway activity (e.g., Akt-mTOR, ERK), which can demonstrate pharmacodynamic engagement of brain-acting drugs.
A recent study demonstrated that ExoSORT-isolated NDEVs detected central Akt-mTOR pathway engagement of liraglutide (a GLP-1 receptor agonist with limited blood-brain barrier penetrance) and pioglitazone (a PPARγ agonist), with baseline Akt(Ser473) phosphorylation predictive of treatment response [10]. The result is a striking proof of concept: NDEV biomarkers can quantify CNS pharmacodynamics from a routine blood draw — a capability that previously required CSF sampling or PET imaging.
5. Disease-Specific Substrate and Metabolite Biomarkers
Many rare neurological diseases are inborn errors of metabolism with characteristic biochemical signatures. These analytes are typically measured by tandem mass spectrometry, immunoassay, or specialized enzymatic methods, and many are incorporated into newborn screening panels [11,12].
Disease | Biomarker | Primary application |
Niemann-Pick disease type C | Lyso-SM-509 | Diagnosis, monitoring |
Krabbe disease | Psychosine | Newborn screening confirmation |
Pompe disease | Glucose tetrasaccharide (Glc4) | Treatment monitoring |
AADC deficiency | 3-O-methyldopa | Diagnosis |
Friedreich’s ataxia | Frataxin | Treatment response |
Wilson disease | Ceruloplasmin, exchangeable copper | Diagnosis, monitoring |
Adrenoleukodystrophy | Very long-chain fatty acids (VLCFAs) | Newborn screening, diagnosis |
Gaucher disease | Glucosylsphingosine (lyso-Gb1) | Treatment monitoring |
6. MicroRNAs and Cell-Free Nucleic Acids
Brain-enriched microRNAs (miR-9, miR-124, miR-128, miR-132) are detectable in plasma and within EVs. While less mature clinically than NfL or GFAP, miRNA panels are being explored in ALS, Huntington’s disease, and pediatric leukodystrophies as potentially disease-specific signatures.
7. Prion-Specific and Seeding Assays
For Creutzfeldt-Jakob disease and other prion disorders, real-time quaking-induced conversion (RT-QuIC) detects misfolded prion protein with extraordinary specificity [14]. Initially CSF- and nasal-brushing-based, blood-based RT-QuIC is an active area of development. The same seeding-assay principle has been extended to alpha-synuclein in Parkinson’s disease and dementia with Lewy bodies, and to tau in primary tauopathies.
Detection Technologies Enabling the Revolution
The clinical utility of any biomarker depends on the assay used to measure it. Several platforms have been transformative:
- Simoa (Single Molecule Array) — digital ELISA with roughly 1,000-fold sensitivity over conventional ELISA, enabling femtogram-level detection of NfL, GFAP, p-tau, and other low-abundance proteins [15].
- Mass spectrometry (LC-MS/MS) — gold standard for small molecules, lipids, and increasingly for protein quantitation (e.g., Aβ42/40 ratio, frataxin).
- Immunoaffinity exosome capture — enables NDEV-specific analysis. Methods include magnetic bead immunoprecipitation, microfluidic devices, and proprietary platforms such as ExoSORT.
- Proximity extension assays (Olink) and aptamer arrays (SomaScan) — enable broad protein panels (1,000–7,000 analytes) for biomarker discovery in small sample volumes.
- Digital PCR and small RNA sequencing — quantify circulating microRNAs and cell-free DNA.
- RT-QuIC and seed amplification assays — amplification-based assays for prion-like proteins.
Clinical Applications Across the Disease Lifecycle
Blood biomarkers serve different purposes at different points in a patient’s journey.
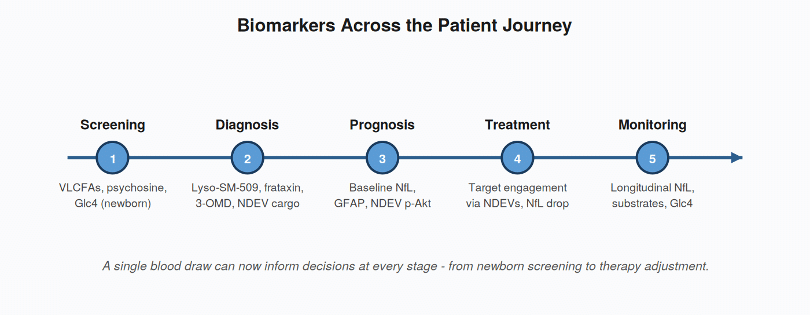
Screening and Diagnosis
Newborn screening for treatable rare conditions (Krabbe, Pompe, MPS-I, ALD) increasingly incorporates dried blood spot biochemical markers. NfL is being explored as a non-specific but sensitive screen for occult neuroaxonal injury in symptomatic patients.
Prognosis and Risk Stratification
Baseline NfL stratifies progression risk in ALS, MS, and SMA. In Huntington’s disease, NfL trajectories help identify mutation carriers nearing manifest disease — an essential capability for trial enrollment.
Pharmacodynamic Monitoring
This is where blood biomarkers shine for rare-disease therapeutics:
- NfL drops within months of effective ALS, SMA, and MS therapies.
- NDEV cargo can demonstrate that a drug reached and engaged its CNS target, informing dose selection and go/no-go decisions in early-phase trials.
- Substrate biomarkers (Glc4, lyso-SM-509, VLCFAs) confirm enzymatic correction in lysosomal and peroxisomal disorders.
Treatment Selection and Adjustment
Emerging precision-medicine approaches use baseline biomarker profiles to select therapy. Baseline phospho-Akt levels in NDEVs, for instance, may help identify patients most likely to respond to mTOR-pathway-modulating drugs [10].
Practical Considerations and Limitations
Despite the enthusiasm, blood biomarkers carry important caveats:
- NfL and GFAP rise in many CNS conditions; an elevated value localizes injury but rarely names the disease.
- Pre-analytical sensitivity. Hemolysis, freeze-thaw cycles, tube type, and time-to-spin all affect results. Standardized SOPs are essential.
- Reference ranges. Values vary by age, sex, BMI, and renal function. Pediatric reference data are still maturing — a particular issue for pediatric-onset rare diseases.
- Assay harmonization. Different platforms can give different absolute values. The international community is developing certified calibrators and reference materials.
- Cost and access. Highly sensitive platforms remain concentrated in academic and specialty centers, though clinical labs are rapidly expanding capacity.
The Road Ahead
Several trends will shape the next five years:
- Multi-analyte panels. Combining NfL, GFAP, p-tau, and disease-specific markers into composite scores will improve specificity and capture different aspects of pathology simultaneously.
- NDEV-based pharmacodynamics. Expect adoption in rare-disease drug development as a standard tool to prove CNS target engagement, particularly for therapeutics with limited or uncertain BBB penetrance.
- Newborn-to-bedside integration. Linking newborn screening, longitudinal NfL monitoring, and gene-therapy outcomes will create unified data streams across a patient’s lifetime.
- Decentralized sampling. Microsampling devices (Tasso, Mitra) enable serial sampling without venipuncture, supporting decentralized trials in geographically dispersed rare-disease populations.
- AI-driven biomarker discovery. Machine learning applied to high-content proteomic and miRNA panels is identifying novel signatures — particularly valuable for ultra-rare conditions where traditional biomarker development is impractical.
Conclusion
Blood biomarkers have moved from research curiosity to clinical and regulatory cornerstone in rare neurological disease. Neurofilament light chain provides a near-universal readout of axonal injury; GFAP captures astrocyte stress; phosphorylated tau and α-synuclein species illuminate proteinopathies; and neuronal-derived extracellular vesicles open a window onto cell-specific intracellular biology, including direct measurement of CNS target engagement of peripheral drugs. Combined with disease-specific substrates and modern detection platforms, these tools are shrinking diagnostic odysseys, accelerating drug development, and bringing precision medicine to patient populations long underserved by rare-disease research.
For clinicians, researchers, and biotech developers working in this space, the message is clear: the brain is no longer hidden. A vial of blood now tells stories that once required the most invasive procedures medicine could offer — and the next wave of innovation will only deepen what blood can reveal.
References
- Khalil M, Teunissen CE, Otto M, et al. Neurofilaments as biomarkers in neurological disorders. Nat Rev Neurol.2018;14(10):577–589. doi:10.1038/s41582-018-0058-z
- Gaetani L, Blennow K, Calabresi P, et al. Neurofilament light chain as a biomarker in neurological disorders. J Neurol Neurosurg Psychiatry. 2019;90(8):870–881. doi:10.1136/jnnp-2018-320106
- Benatar M, Wuu J, Andersen PM, et al. Neurofilament light: a candidate biomarker of presymptomatic ALS and phenoconversion. Ann Neurol. 2018;84(1):130–139. doi:10.1002/ana.25276
- Byrne LM, Rodrigues FB, Blennow K, et al. Neurofilament light protein in blood as a potential biomarker of neurodegeneration in Huntington’s disease. Lancet Neurol. 2017;16(8):601–609. doi:10.1016/S1474-4422(17)30124-2
- Olsson B, Alberg L, Cullen NC, et al. NFL is a marker of treatment response in children with SMA treated with nusinersen. J Neurol. 2019;266(9):2129–2136. doi:10.1007/s00415-019-09389-8
- Miller TM, Cudkowicz ME, Genge A, et al. Trial of antisense oligonucleotide tofersen for SOD1 ALS. N Engl J Med.2022;387(12):1099–1110. doi:10.1056/NEJMoa2204705
- Heller C, Foiani MS, Moore K, et al. Plasma glial fibrillary acidic protein is raised in progranulin-associated frontotemporal dementia. J Neurol Neurosurg Psychiatry. 2020;91(3):263–270. doi:10.1136/jnnp-2019-321954
- Janelidze S, Mattsson N, Palmqvist S, et al. Plasma P-tau181 in Alzheimer’s disease: relationship to other biomarkers, differential diagnosis, neuropathology and longitudinal progression. Nat Med. 2020;26(3):379–386. doi:10.1038/s41591-020-0755-1
- Mustapic M, Eitan E, Werner JK, et al. Plasma extracellular vesicles enriched for neuronal origin: a potential window into brain pathologic processes. Front Neurosci. 2017;11:278. doi:10.3389/fnins.2017.00278
- Evers M, Watson AT, Abbasi M, Haque K, Verma R, Eitan E, Rasgon NL. ExoSORT NDEV biomarkers detect central Akt-mTOR engagement of liraglutide and pioglitazone. J Clin Endocrinol Metab. 2026 (advance article). doi:10.1210/clinem/dgag176
- Vanderver A, Wolf NI, Patterson MC, et al. Newborn screening and the leukodystrophies. 2020;95(22):e3007–e3019. doi:10.1212/WNL.0000000000010696
- Giese AK, Mascher H, Grittner U, et al. A novel, highly sensitive and specific biomarker for Niemann-Pick type C1 disease. Orphanet J Rare Dis. 2015;10:78. doi:10.1186/s13023-015-0274-1
- Foiani MS, Cicognola C, Ermann N, et al. Searching for novel cerebrospinal fluid biomarkers of tau pathology in frontotemporal dementia. J Neurol Neurosurg Psychiatry. 2019;90(7):740–746. doi:10.1136/jnnp-2018-319713
- Orrù CD, Groveman BR, Hughson AG, et al. RT-QuIC assays for prion disease detection, diagnostics and therapeutics. Methods Mol Biol. 2017;1658:185–203. doi:10.1007/978-1-4939-7244-9_14
- Wilson DH, Rissin DM, Kan CW, et al. The Simoa HD-1 Analyzer: a novel fully automated digital immunoassay analyzer with single-molecule sensitivity and multiplexing. J Lab Autom. 2016;21(4):533–547. doi:10.1177/2211068215589580

Leave a Reply