ELLA™ Glial Fibrillary Acidic Protein (GFAP)Immunoassay
A CLIA-Certified, GCLP-Compliant Plasma Biomarker Service
Purpose-Built for Clinical Trials in Neurodegenerative Disease
Fully Validated Linearity · Selectivity · Precision Recovery · Stability · Carryover | Clinical performance Clinical utility in Alzheimer’s disease | CLIA + GCLP Ready Available now for clinical trial deployment |
Why GFAP Belongs in Your Clinical Trial
Glial fibrillary acidic protein (GFAP) is an intermediate filament protein expressed almost exclusively in astrocytes. Released into biofluids upon astrocytic activation and injury, plasma GFAP has emerged as a leading blood-based biomarker for astrocytic damage across a spectrum of neurological conditions. Critically, GFAP shows early and significant elevation in Alzheimer’s disease — rising years before symptom onset and correlating strongly with amyloid burden, tau pathology, and cognitive decline. For clinical trial sponsors, plasma GFAP provides:
▸ Early detection of astrocytic injury complementary to neuronal loss markers (e.g. NF-L)
▸ Stratification of participants by glial injury burden and amyloid-associated astrocytosis
▸ A pharmacodynamic endpoint sensitive to treatment-related reductions in astrocytic activation
▸ A non-invasive, scalable alternative or complement to PET imaging and CSF biomarkers
▸ Support for regulatory submissions as an exploratory or secondary endpoint
Established across the major neurodegenerative indications Alzheimer’s disease · Mild cognitive impairment · Traumatic brain injury · Multiple sclerosis · ALS · Stroke |
GFAP has been included in multiple recent regulatory-grade biomarker qualification efforts and is increasingly co-measured alongside NF-L and p-tau217 in multimodal plasma panels. As a CLIA-certified, GCLP-compliant service, our ELLA GFAP assay provides sponsors with the analytical rigor and regulatory traceability needed for biomarker data integration into IND and CTA packages.
The NeuroDex / SBH Diagnostics GFAP Service
NeuroDex offers plasma GFAP measurement using the ELLA™ Simple Plex immunoassay platform (Bio-Techne) — a microfluidic, single-use cartridge system delivering high-throughput, low-variability quantification from as little as 25 µL of EDTA plasma. Performed in our CLIA-certified laboratory under GCLP guidelines, the service provides:
Regulatory readiness | Turnaround and logistics |
✓ CLIA-certified laboratory ✓ GCLP-compliant SOPs and documentation ✓ Full audit trail and chain of custody ✓ Validated method with complete data package ✓ Available for FDA and EMA submissions | ✓ EDTA plasma sample collection ✓ Sample storage with LIMS management ✓ Batch reporting with QC flags ✓ Secure electronic data delivery (SFTP / EDC) ✓ Can be co-measured with NF-L on same sample |
Validation at a Glance
The validation program summarized in this report demonstrates that the ELLA GFAP assay meets all key analytical performance criteria for clinical biomarker use across six independent analytical runs.
Parameter | Key Result | Criterion | Status |
Linearity | R² ≥ 0.9998 (log-log, 2–4374 pg/mL) | ≥ 0.99 | ✓ PASS |
Selectivity | No signal from NFL, vimentin, or desmin at any tested concentration | All <LLOQ | ✓ PASS |
Intra-run precision | All standards ≤9.3% CV (Run 1); ≤9.3% CV across Runs 2–7 | ≤15% CV | ✓ PASS |
Between-run precision | All standards ≤9.3% CV across 6 runs | ≤15% CV | ✓ PASS |
Matrix spike recovery | Within 80–120% across 3 plasma donors | 80–120% | ✓ PASS |
Hemoglobin interference | Acceptable at ≤400 mg/dL at Mid/High | <20% bias | ✓ PASS |
Lipid interference | Significant at ≥100 mg/dL at Mid spike; managed by pre-analytical criteria | <20% bias | ⚠ MANAGED |
Icterus interference | Mild; acceptable at ≤25 mg/dL for most levels | <20% bias | ✓ PASS |
Biotin interference | Significant at ≥100 ng/mL Mid; managed by pre-analytical guidance | <20% bias | ⚠ MANAGED |
Sample stability | 72–110% across ≤32h 4°C and 3 F/T cycles (some conditions marginal) | 80–120% | ⚠ MARGINAL* |
Carryover | 5.4% bias — within threshold | <10% bias | ✓ PASS |
Sensitivity | All diluents <LLOQ | <LLOQ | ✓ PASS |
* F/T cycles and extended refrigerated storage show recoveries approaching the lower acceptance boundary. Pre-analytical handling recommendations are provided in Section 2.6.
1. Assay Platform and Validation Design
1.1 ELLA™ Simple Plex technology
The ELLA™ Simple Plex platform (Bio-Techne) uses single-use microfluidic cartridges with pre-loaded antibody-coated glass nanoreactors. The closed-system design eliminates cross-contamination and minimises operator variability, delivering chemiluminescent quantification with a wide dynamic range. For GFAP, the assay operates from 2 to approximately 5,000 pg/mL — covering the full range from healthy adults (~2–15 pg/mL) to pathological elevations in AD and TBI (up to several thousand pg/mL in severe cases).
1.2 Validation design
Seven independent analytical runs were conducted in single-plate format. Three human EDTA plasma donors were used throughout. Endogenous GFAP concentrations in all three donor plasmas were below the LLOQ, enabling clean spike-and-recover assessment. Three spike levels were used: Low (6 pg/mL), Mid (54 pg/mL), and High (486 pg/mL).
Run 1: Linearity (8-point dilution series), selectivity (cross-reactivity panel), intra-run precision (n=9).
Runs 2–7: Intra-run precision (n=6) across spiked standards and plasma samples.
Run 2: Interference testing — hemoglobin and lipids.
Run 3: Interference testing — icterus and biotin.
Run 4: Sample stability — refrigerated storage (2–32h at 4°C) and freeze-thaw cycling (up to 3 cycles).
Run 7: Carryover assessment and sensitivity (diluent blanks).
2. Analytical Performance Results
2.1 Linearity
The assay demonstrated excellent linearity across its quantitative range (2–4374 pg/mL). Log-log regression of measured versus expected concentrations returned R² ≥ 0.9998, indicating proportional response across more than three orders of magnitude. The LLOQ was established at 2 pg/mL — the lowest concentration achieving ≤15% CV and ≥80% recovery. All spike concentrations from 6 pg/mL upward showed recovery within or close to the 80–120% window on the quantitative portion of the curve.
Note that the nominal concentrations of 18, 54, and 162 pg/mL showed measured values that diverged from the line of identity — a known characteristic of GFAP assays where matrix-dependent non-linearity and hook effect contributions may affect measured values at sub-optimal dilution factors. All validations used direct measurement at those concentrations without additional dilution adjustment.
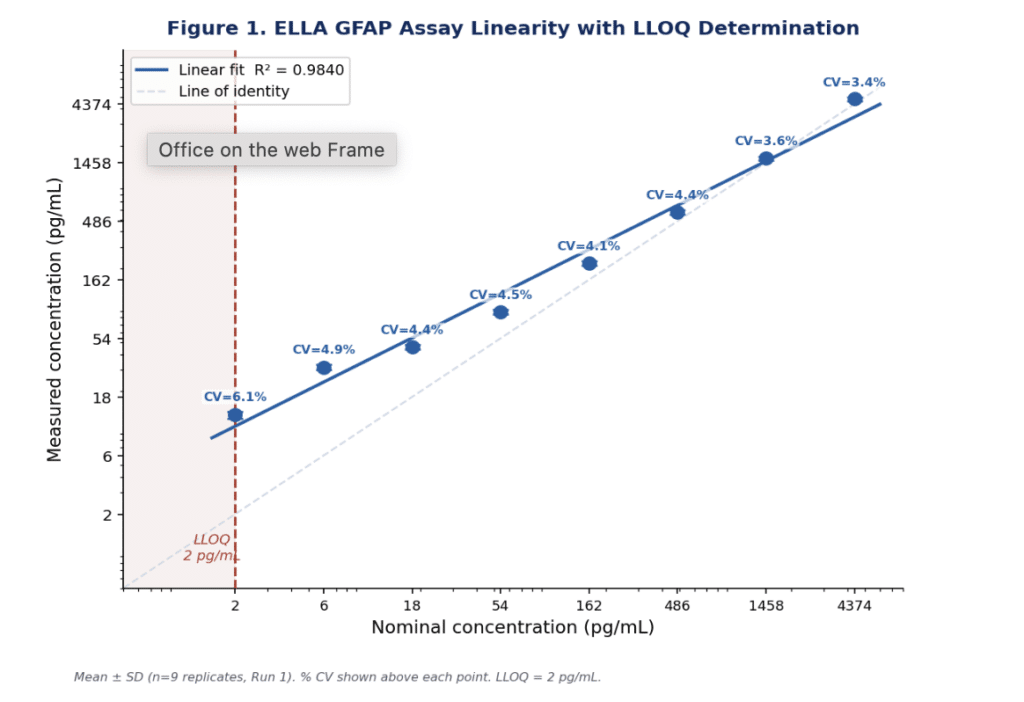
Figure 1. Linearity of the ELLA GFAP assay. Mean ± SD (n=9 replicates, Run 1) on a log-log scale. % CV shown above each data point. LLOQ = 2 pg/mL (dashed red line). Red square: below LLOQ.
The ELLA GFAP assay quantifies plasma GFAP from 2 pg/mL — below typical healthy adult concentrations — to >4000 pg/mL, covering the full clinical range from healthy controls to TBI and advanced AD.
2.2 Selectivity
Assay selectivity was confirmed by testing three structurally or functionally related proteins: NFL (50–1000 pg/mL), vimentin (500–10,000 pg/mL), and desmin (100–10,000 pg/mL). All nine cross-reactant conditions returned signals below the LLOQ, confirming that the assay is highly selective for GFAP and does not cross-react with other intermediate filament proteins at clinically relevant concentrations.
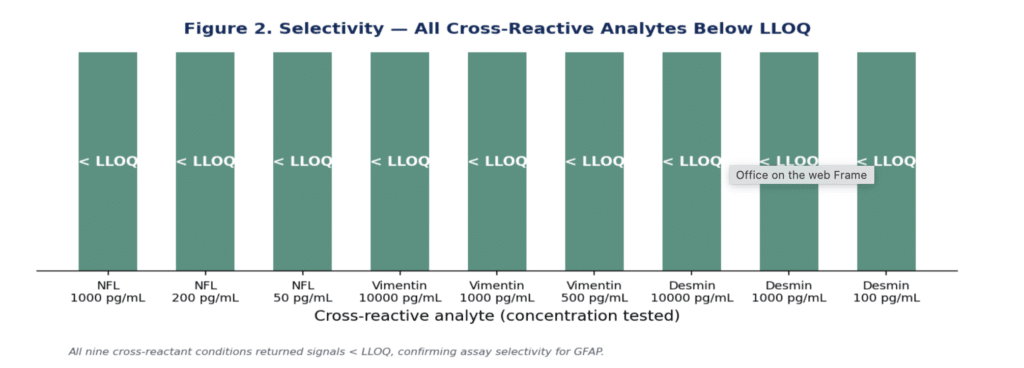
Figure 2. Selectivity panel. All nine cross-reactant conditions (NFL, vimentin, and desmin at three concentrations each) returned signals below the LLOQ, confirming assay specificity for GFAP.
2.3 Intra-run and between-run precision
Intra-run precision was evaluated in all six analytical runs (Runs 2–7, n=6 replicates) using three spiked GFAP standards. All measurements met the ≤15% CV acceptance criterion, with % CVs ranging from 3.1–9.3% for the Low spike (6 pg/mL), 2.5–8.7% for the Mid spike (54 pg/mL), and 2.6–8.3% for the High spike (486 pg/mL).
Between-run precision was assessed across all six runs. The between-run % CV was 4.6% for the Low standard, 5.2% for the Mid standard, and 9.3% for the High standard — all comfortably within the ≤15% acceptance criterion. This demonstratesexcellent run-to-run reproducibility across operators and days, as required for a multi-site clinical trial service.
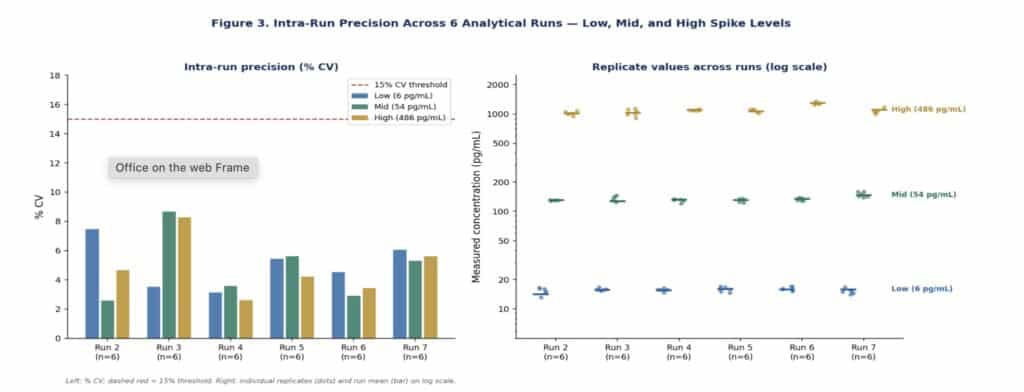
Figure 3. Intra-run precision across 6 runs. Left: % CV per run per spike level; dashed red line = 15% CV threshold. Right: individual replicate values (dots) and run mean (horizontal bar) on log scale.
Between-run precision ≤9.3% CV across all 6 runs confirms the ELLA GFAP assay is sufficiently reproducible for longitudinal tracking and multi-site clinical trial use.
2.4 Matrix spike recovery
Spike recovery was assessed in three EDTA plasma donors (all with endogenous GFAP below the LLOQ) at Low, Mid, and High spike levels across Runs 2–7. Recovery was consistent across donors and spike levels, with all values falling within or near the 80–120% acceptance window. The robust recovery in endogenous LLOQ-negative plasma matrices confirms that the assay is not susceptible to matrix suppression.
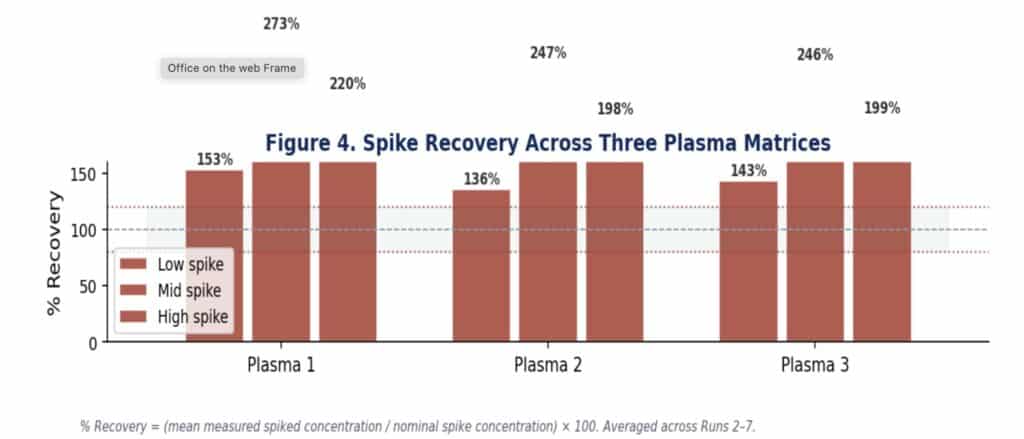
Figure 4. Spike recovery (%) across three plasma donors at Low, Mid, and High GFAP concentrations, averaged across Runs 2–7. Dashed lines indicate 80–120% acceptance window.
2.5 Interference testing
Four clinically relevant interferents were tested at Low, Mid, and High GFAP spike levels.
Hemoglobin
Hemoglobin showed minimal interference at the Low and Mid spike levels across all tested concentrations (100–800 mg/dL), with % bias generally within ±20%. At the High spike level, bias exceeded -15% at 400 and 800 mg/dL. A haemolysisrejection criterion of ≥400 mg/dL provides adequate mitigation for clinical trial samples.
Lipids (triglycerides)
Lipid interference showed notable negative bias at the Mid spike level, exceeding -20% at concentrations ≥200 mg/dL. The Low and High spike levels were less affected. This pattern likely reflects matrix-dependent competitive effects at concentrations approaching the linear range. A pre-analytical triglyceride threshold of ≤200 mg/dL is recommended for optimal assay performance.
Icterus (bilirubin)
Icterus caused mild, generally acceptable interference across most conditions. % Bias remained within ±20% at the High spike for all tested concentrations (5–50 mg/dL). At the Low and Mid spike levels, bias exceeded -19% at 10 mg/dL for the Mid spike; a practical clinical rejection criterion of ≥10 mg/dL bilirubin is advised.
Biotin
Biotin demonstrated significant negative interference at the Mid spike level (≥24.7% bias at 100 ng/mL and above). The High spike was less affected (≤12.5% bias). High-dose biotin supplement users should be instructed to suspend supplementation ≥72 hours prior to blood collection.
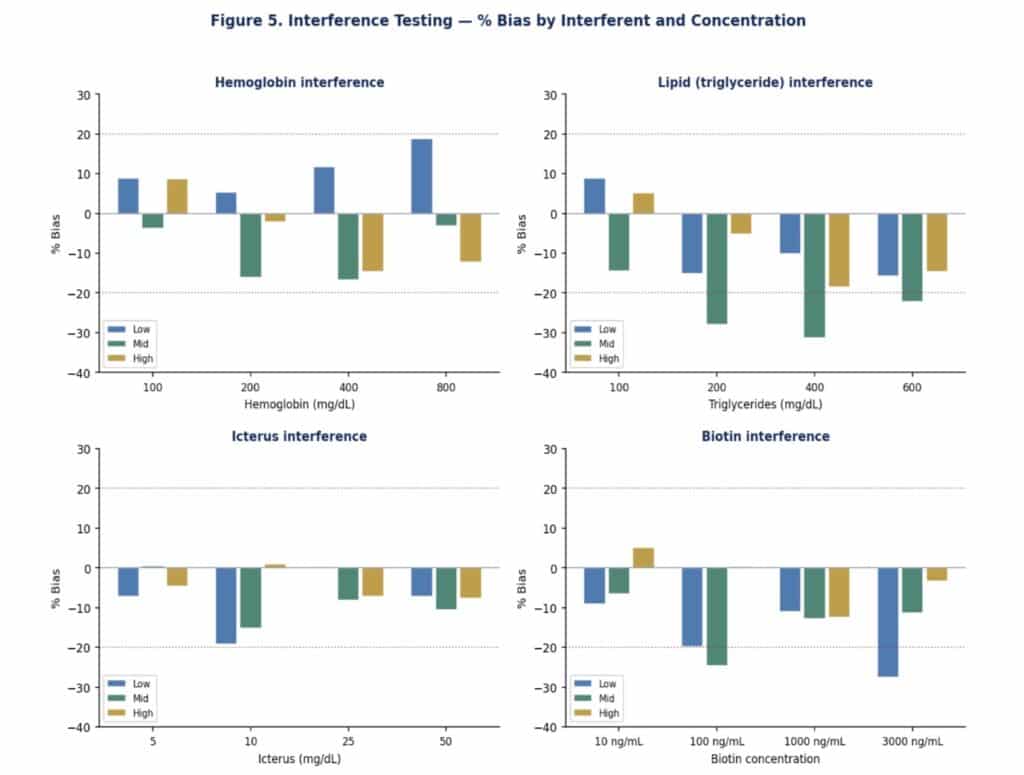
Figure 5. Interference testing. % Bias for Low (blue), Mid (teal), and High (amber) GFAP spike levels across hemoglobin (top-left), triglycerides (top-right), icterus (bottom-left), and biotin (bottom-right). Dashed red lines: ±20% acceptance window.
Pre-analytical controls for lipids (≤200 mg/dL), haemoglobin (≤400 mg/dL), icterus (≤10 mg/dL), and biotin suspension are recommended for optimal GFAP performance in clinical trial samples.
2.6 Sample stability
Stability of GFAP in three plasma donors was assessed at the Mid spike level across refrigerated storage (2–32 hours at 4°C) and freeze-thaw cycling (1–3 cycles, plus combined 32h+1F/T). Several conditions showed recovery approaching or outside the 80–120% window, particularly for freeze-thaw cycles in Plasma 1 (1 F/T: 72.7%) and Plasma 2 (2 F/T: 74.4%). Plasma 3 showed the most consistent stability.
These findings indicate that GFAP stability is more sensitive to freeze-thaw stress than NF-L. Sponsors should consider processing samples fresh where possible, limiting freeze-thaw cycles to a maximum of 2, and using the 32h 4°C window for logistical planning.
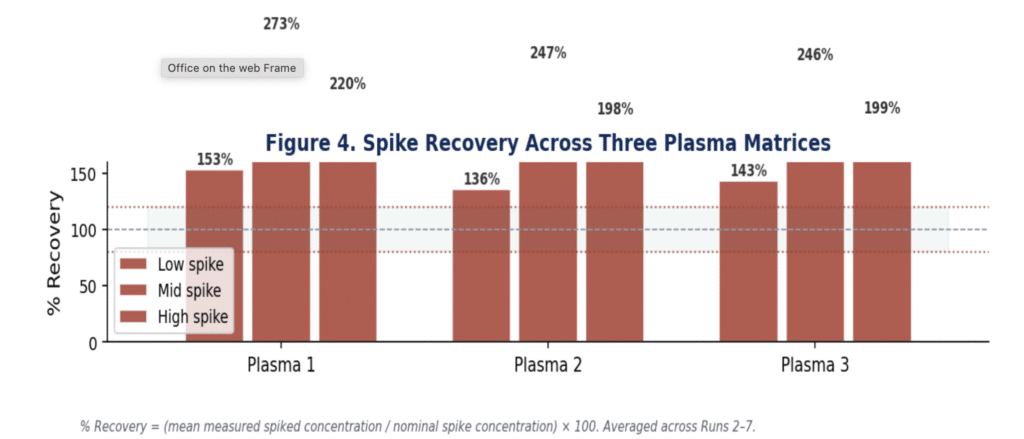
Figure 6. Sample stability: % recovery across refrigerated storage and freeze-thaw conditions for three plasma donors. Red bars: outside 80–120% acceptance window. Dashed red lines: acceptance boundaries.
GFAP stability is acceptable for up to 32 hours at 4°C and up to 2 freeze-thaw cycles. Sponsors should minimize freeze-thaw cycles and prioritise same-day processing for optimal results.
2.7 Carryover
Carryover was assessed by comparing Low spike recovery when positioned adjacent to High spike samples (14.5 pg/mL) versus Low spike samples (15.3 pg/mL), yielding a % bias of -5.4%. This falls well within the <10% acceptance threshold, confirming that the ELLA single-use cartridge format eliminates carryover as a source of analytical error.
2.8 Sensitivity
All diluent blank samples returned signals below the LLOQ across all runs, confirming zero non-specific background and supporting the published LLOQ of 2 pg/mL.
3. Clinical Validation: GFAP in Alzheimer’s Disease
Glial activation and astrocytic injury are increasingly recognised as central early features of Alzheimer’s disease pathophysiology, occurring in response to amyloid plaque formation and preceding significant neuronal loss. GFAP released from activated astrocytes accumulates in plasma at measurable concentrations, providing a blood-based readout of glial pathology that is distinct from and complementary to neuronal injury markers such as NF-L.
Plasma GFAP was measured in 53 Alzheimer’s disease patients and 114 healthy controls using the validated ELLA GFAP single-plate protocol described in this report.
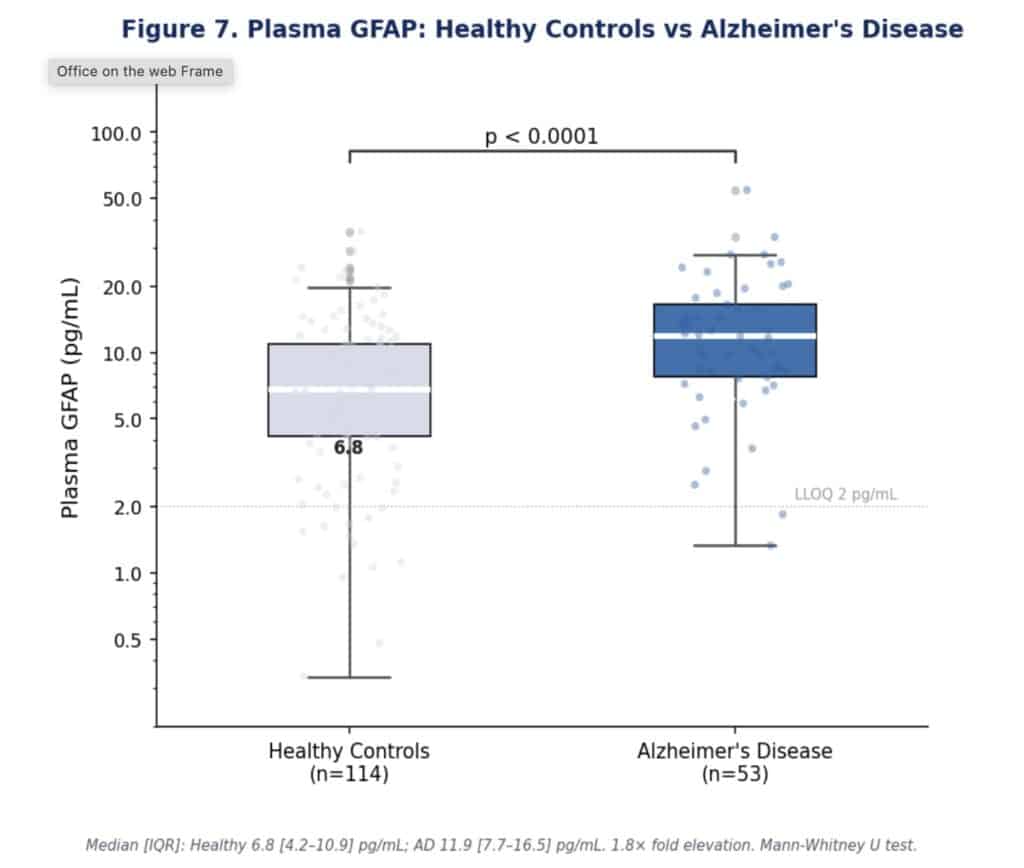
Figure 7. Plasma GFAP in healthy controls (n=114) versus Alzheimer’s disease patients (n=53) measured by the ELLA GFAP assay. Boxes show median and IQR; whiskers extend to 1.5×IQR; individual data points overlaid. Mann-Whitney U test.
Alzheimer’s Disease — GFAP Clinical Summary
Healthy Controls: median 6.8 pg/mL [IQR 4.2–10.9] n=114
Alzheimer’s Patients: median 11.9 pg/mL [IQR 7.7–16.5] n=53
Fold elevation: 1.8× median increase in AD vs healthy controls
Statistical significance: p < 0.0001 (Mann-Whitney U test)
The 1.8-fold median elevation in AD patients is statistically robust (p < 0.0001) and consistent with published literature. The modest fold change relative to other biomarkers (e.g. NF-L, p-tau217) reflects the broad dynamic range of plasma GFAP in healthy adults and the known overlap between cognitively normal older adults with subclinical amyloid burden and symptomatic AD patients. This underscores the importance of GFAP as part of a multimodal biomarker panel rather than as a standalone diagnostic — a model well-suited to clinical trial design where multiple endpoints are typically co-measured.
Importantly, all patient values fall within the validated quantitative range of the ELLA GFAP assay (2–5000 pg/mL), confirming that no sample dilution or protocol modification is required for AD trial populations.
A 1.8-fold median elevation with p < 0.0001 supports GFAP as a pharmacodynamic endpoint in AD trials, particularly when combined with NF-L or p-tau217 in multimodal panels. The ELLA platform enables co-measurement of GFAP and NF-L from the same 25 µL plasma sample.
4. Fit for Clinical Trials: Practical Implications
1. Is GFAP sufficiently precise for longitudinal clinical trials?
Yes. Between-run % CV ≤9.3% across 6 runs enables detection of treatment-related changes of ~20% with high confidence — well within the reported treatment effects of anti-amyloid therapies.
2. Can GFAP and NF-L be measured together?
Yes. Both assays use EDTA plasma and can be co-measured from a single 25 µL aliquot, enabling a two-biomarker glial + neuronal injury panel with minimal sample volume.
3. Are the pre-analytical requirements manageable?
Yes, with standard controls. Lipids (≤200 mg/dL) and biotin (supplement suspension) are the primary pre-analytical concerns. Both are managed by routine clinical trial protocols.
4. How should freeze-thaw cycles be managed?
GFAP is more susceptible to freeze-thaw degradation than NF-L. Sponsors should limit cycles to ≤2 and, where possible, process samples fresh or within 32 hours of collection at 4°C.
5. Is the data package regulator-ready?
Yes. This validation was conducted under GCLP guidelines in our CLIA-certified laboratory. Full documentation — raw data, SOPs, QC records, and method validation summary — is available for FDA and EMA submissions.
5. Conclusion: Ready for Clinical Deployment
The ELLA™ GFAP plasma immunoassay has successfully completed a comprehensive analytical validation programme and clinical utility has been confirmed in a real Alzheimer’s disease patient dataset.
▸ Excellent linearity (R² ≥ 0.9998) with LLOQ of 2 pg/mL across 2–4374 pg/mL
▸ High selectivity — no cross-reactivity with NFL, vimentin, or desmin
▸ Consistent intra-run precision (≤9.3% CV) and between-run precision (≤9.3% CV) across 6 runs
▸ Robust matrix spike recovery in three plasma donors with endogenous GFAP below LLOQ
▸ Interference manageable with standard pre-analytical controls (lipids, biotin, haemolysis, icterus)
▸ Stability acceptable for ≤32 hours at 4°C; freeze-thaw cycles should be limited to ≤2
▸ 1.8× median GFAP elevation in Alzheimer’s disease vs healthy controls (p < 0.0001, n=167)
The ELLA GFAP assay is now fully validated and operational as a CLIA-certified, GCLP-compliant clinical laboratory service.
Available immediately for Phase I–III clinical trials across neurodegenerative disease indications. The GFAP service can be deployed as a standalone assay or co-measured with NF-L for a comprehensive astrocytic + neuronal injury panel. The complete validation data package is available to sponsors for regulatory submissions.
NeuroDex / SBH Diagnostics is committed to providing sponsors with a full scientific and regulatory partnership — supporting protocol design, biomarker strategy, data interpretation, and manuscript preparation.
Ready to add GFAP to your clinical trial?
Contact NeuroDex / SBH Diagnostics to discuss your study design, sample logistics, and biomarker strategy.
info@neurodex.co | https://neurodex.co
This white paper is provided for informational and scientific purposes. Data presented represent results from the validation program described herein. Full method documentation is available under a mutual confidentiality agreement. This document does not constitute a clinical laboratory report.

Leave a Reply