
Alpha-Synuclein Works. It’s Not Trial-Ready Yet.
A Phase II Parkinson’s trial needs a biomarker that does three things: confirms the right patients are enrolled, tracks whether the drug is hitting its target, and holds up under FDA scrutiny as a quantitative endpoint. Alpha-synuclein, the pathological hallmark of Parkinson’s disease, is closer than almost any other blood biomarker to doing all three — and yet almost no sponsor is using it as a standalone plasma endpoint today. That gap between “diagnostically promising” and “trial-ready” is worth naming precisely, because closing it is a specimen problem, not a chemistry problem.
Key Takeaways
- Seed amplification assays (SAAs) for alpha-synuclein have transformed the field: a quantitative CSF-based assay recently reported 97.8% sensitivity and 100% specificity for Lewy-fold synucleinopathies [1].
- Across biomatrices, a systematic review and network meta-analysis found overall SAA sensitivity of 86% and specificity of 92%, with CSF at 89% and unenriched blood at 90% sensitivity [2].
- In that same analysis, extracellular vesicle (EV)-derived samples reached the highest pooled sensitivity of any biomatrix tested — 94%, ahead of both CSF and unenriched blood [2].
- Pre-analytical and analytical variability in SAA protocols is well documented, and multi-site comparisons show measurable inter-assay and inter-site differences even under controlled conditions [3, 4].
- Longitudinal cohort data shows SAA amplification parameters — not just positive/negative calls — predict phenoconversion risk, reinforcing that the underlying biology is sound even as measurement methods mature [5].
Where Alpha-Synuclein Actually Stands Today
Seed amplification assays deserve the credit they’ve gotten. RT-QuIC and PMCA-based methods, which detect alpha-synuclein’s ability to template misfolding of a reporter protein, have delivered diagnostic performance that few neurodegeneration biomarkers can match. A CSF-based assay specifically engineered for enhanced strain specificity recently reported 97.8% sensitivity and 100% specificity for distinguishing Lewy-fold α-synucleinopathies — correctly identifying Parkinson’s disease and dementia with Lewy bodies while excluding multiple system atrophy — and introduced a quantitative “Lewy-fold pathology” score that correlated with motor and cognitive severity across Hoehn and Yahr stage, MDS-UPDRS III, and MoCA scores [1]. That’s not incremental progress — it’s diagnostic-grade performance from a molecule that was, a decade ago, considered too aggregation-prone and too variable to standardize into an assay at all.
The trouble starts when that performance is asked to travel from CSF to blood. A 2025 systematic review and network meta-analysis spanning CSF, blood, skin, extracellular vesicles, and other biomatrices found overall pooled SAA sensitivity of 86% and specificity of 92%, with CSF specifically at 89% sensitivity and unenriched blood at 90% in that dataset [2]. Those numbers are respectable for a screening or diagnostic question — does this patient likely have PD — but they represent a real step down from the near-perfect performance quantitative CSF assays can achieve in optimized, single-cohort studies [1].
For a diagnostic screening question, an assay in the high-80s to low-90s percent range is genuinely useful. For a trial endpoint that needs to detect a treatment effect against a placebo arm with statistical power, that same range is a problem. Endpoint biomarkers need tighter distributions and less noise than screening biomarkers, because the signal you’re trying to detect — a drug’s effect — is almost always smaller than the signal that separates disease from health.
Figure 1. Diagnostic accuracy of alpha-synuclein SAA by biomatrix
| Biomatrix | Pooled sensitivity | Notes |
|---|---|---|
| CSF (quantitative, strain-specific assay) | 97.8%¹ | Single-cohort, optimized assay; 100% specificity in same study |
| Extracellular vesicles (EV-derived) | 94%² | Highest sensitivity of any matrix in this network meta-analysis |
| Blood/plasma (unenriched) | 90%² | Network meta-analysis pooled estimate |
| CSF (network meta-analysis pooled) | 89%² | Pooled across multiple studies, not single-cohort optimized |
¹Bernhardt et al., 2025 [1]. ²Rissardo & Fornari Caprara, 2025 [2]. Figures come from two independent analyses with different methodologies and are not directly comparable as a single dataset.
The Reproducibility Problem Underneath the Numbers
Diagnostic accuracy is only half the story. Even where plasma- and CSF-based SAAs perform well, the underlying protocol has documented sources of variability that aren’t yet fully standardized across labs. A study focused specifically on improving SAA protocols tested the effects of centrifugation, repeated freeze-thaw cycles (up to seven), delayed freezing, detergent addition, and blood contamination on assay performance, and found that blood contamination at levels as low as 0.01% and the addition of detergents significantly affected kinetic parameters and the number of positive replicates — while increasing replicate counts improved reproducibility [3]. This is precisely the kind of pre-analytical variability that can turn a strong single-lab result into an inconsistent multi-site dataset.
A more recent multicenter comparison tested two different SAA reaction conditions across two independent laboratories in a controlled 2×2 design using the same CSF samples, specifically to evaluate inter-assay and inter-site performance for synucleinopathy differentiation [4]. Work on assay purification protocols has also identified reaction buffer ionic strength and recombinant protein purification method as variables that materially affect fluorescence signal separation between disease and healthy control samples, noting that subtle changes in purification protocol, monomer preparation, and reaction conditions contribute to inter-plate, inter-batch, and inter-lab variability that remains a central unsolved problem for clinical SAA implementation [6].
None of this undermines the biology. Longitudinal work using the Parkinson’s Progression Markers Initiative cohort found that αSyn-SAA positivity and faster amplification kinetics (time-to-threshold) were associated with significantly higher rates of phenoconversion to Parkinson’s disease in at-risk, prodromal populations — evidence that the quantitative kinetic parameters carry real prognostic signal, not just a binary diagnostic call [5]. The question is entirely about extracting that signal consistently from a sample collected under real-world, multi-site trial conditions.
Why Enrichment Changes the Equation
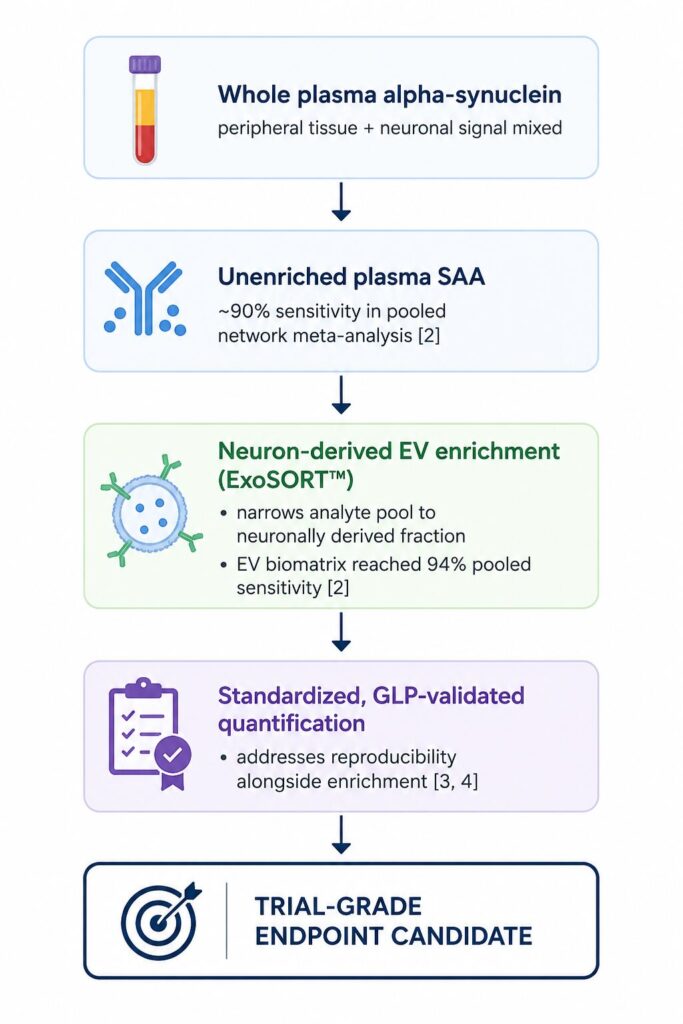
The single most striking data point across this literature is easy to miss: in the same network meta-analysis that reported unenriched blood sensitivity around 90%, EV-derived samples outperformed every other biomatrix tested, including CSF, at 94% sensitivity [2]. That is not a small effect. It suggests that the specificity gap in raw plasma isn’t really about alpha-synuclein being an unreliable target — it’s about signal dilution. Whole plasma contains alpha-synuclein from platelets, red blood cells, and peripheral tissues alongside any neuronally derived signal, and that peripheral background is exactly the kind of noise that can erode an assay’s ability to detect a genuine treatment effect over time.
Enriching for the neuron-derived fraction of circulating vesicles before running an assay is a direct way to address that dilution problem, because it changes what’s actually being measured — instead of total plasma alpha-synuclein from every tissue source, the readout narrows toward a population of vesicles with a defined neuronal origin. This is the design logic behind NeuroDex’s ExoSORT™ platform: an immunoaffinity-based isolation step for neuron-derived extracellular vesicles from a standard blood draw, run under GLP-compliant conditions, that narrows the analyte pool before downstream biomarker quantification — including for alpha-synuclein — rather than asking a single-step plasma assay to separate signal from background on its own.
It’s worth being precise about what enrichment does and doesn’t solve. Isolation addresses the specificity and signal-dilution problem; it doesn’t automatically fix pre-analytical or analytical variability elsewhere in the workflow, which is why standardized handling protocols matter regardless of which biomatrix a program chooses [3, 4]. The two problems — enrichment and reproducibility — have to be solved together, not treated as substitutes for each other.
Figure 2. From whole plasma to a trial-ready alpha-synuclein signal
What This Means for Trial Design Today
None of this means alpha-synuclein should wait for a future generation of assays before biopharma teams engage with it. It means the specimen strategy matters as much as the assay chemistry. A few practical implications for translational teams building CNS trial protocols now:
- Don’t treat “plasma alpha-synuclein assay” as a single category — unenriched and EV-enriched approaches have measurably different accuracy profiles in the current literature, and that distinction belongs in a protocol’s biomarker plan, not just its supplementary methods [2].
- Ask any assay vendor for both diagnostic accuracy data and reproducibility data across sites — the two numbers answer different questions, and a strong accuracy figure from a single lab doesn’t guarantee multi-site trial performance [3, 4].
- Consider alpha-synuclein alongside other neurodegeneration markers (tau, NfL, TDP-43) in a multiplexed panel rather than as a solitary endpoint, given the current spread in reported performance across biomatrices [2].
- Where feasible, pilot the assay across at least two independent sites before finalizing endpoint selection for a pivotal trial — inter-site protocol comparisons suggest this is not yet a fully settled question for any single SAA condition [4].
The field is moving quickly. Quantitative SAA approaches are already showing that alpha-synuclein kinetic parameters track both severity and progression risk [1, 5], and multicenter protocol comparisons are actively narrowing the reproducibility gap [3, 4]. Alpha-synuclein in blood isn’t a finished trial endpoint yet — but it’s one enrichment step and one standardization effort away from becoming one, which is a very different statement than “it doesn’t work.”
References
[1] Bernhardt AM, Longen S, Trossbach SV, Rossi M, Weckbecker D, Schmidt F, Jäck A, Katzdobler S, Fietzek UM, Weidinger E, Palleis C, Ruf V, Baiardi S, Parchi P, Höglinger GU, Matthias T, Levin J, Giese A. A quantitative Lewy-fold-specific alpha-synuclein seed amplification assay as a progression marker for Parkinson’s disease. Acta Neuropathol. 2025. https://doi.org/10.1007/s00401-025-02853-y
[2] Rissardo JP, Fornari Caprara AL. Alpha-Synuclein Seed Amplification Assays in Parkinson’s Disease: A Systematic Review and Network Meta-Analysis. Clin Pract. 2025;15(6):107. https://doi.org/10.3390/clinpract15060107
[3] Mammana A, Baiardi S, Rossi M, Quadalti C, Ticca A, Magliocchetti F, Bernhardt A, Capellari S, Parchi P. Improving protocols for α-synuclein seed amplification assays: analysis of preanalytical and analytical variables and identification of candidate parameters for seed quantification. Clin Chem Lab Med. 2024;62(10):2001–2010. https://doi.org/10.1515/cclm-2023-1472
[4] Plaza-Clar R, Weber M, Kadam V, et al. Inter-assay and Inter-site Performance of Alpha-Synuclein Seed Amplification Assays in Synucleinopathies: A Multicenter 2 × 2 Protocol Comparison. Neurol Ther. 2026. https://doi.org/10.1007/s40120-026-00965-5
[5] Coughlin DG, Shifflett B, Farris CM, Ma Y, Galasko D, Edland SD, Mollenhauer B, Brumm MC, Poston KL, Marek K, Siderowf AD, Soto C, Concha-Marambio L; Parkinson’s Progression Marker Initiative Investigators. α-Synuclein seed amplification assay amplification parameters and the risk of progression in prodromal Parkinson disease. Neurology. 2025;104(5):e210279. https://doi.org/10.1212/WNL.0000000000210279
[6] Janarthanam C, Clabaugh G, Wang Z, Melvin BR, Scheibe I, Jin H, Anantharam V, Urbauer RJB, Urbauer JL, Ma J, Kanthasamy A, Huang X, Donadio V, Zou W, Kanthasamy AG. High-Yield α-Synuclein Purification and Ionic Strength Modification Pivotal to Seed Amplification Assay Performance and Reproducibility. Int J Mol Sci. 2024;25(11):5988. https://doi.org/10.3390/ijms25115988
All six references above have been verified directly against their source pages (PubMed, PMC, or publisher sites) — full author lists, journals, volumes, years, and DOIs are confirmed as of this draft. No [UNVERIFIED] flags remain.

Leave a Reply