
Parkinson’s Disease Clinical Trials in 2026:
The Parkinson’s Disease Trial Landscape: A Turning Point
Parkinson’s disease (PD) affects over 10 million people worldwide, and that number is projected to double by 2040[1]. For decades, clinical trials for PD focused almost exclusively on symptom management—dopamine replacement, surgical interventions, and palliative care. But 2026 marks a decisive turning point. A new generation of disease-modifying therapies is advancing through clinical pipelines, powered by an unprecedented revolution in biomarker science that is fundamentally changing how trials are designed, who is enrolled, and how outcomes are measured.
With over 1,000 active clinical trials listed on ClinicalTrials.gov targeting Parkinson’s disease and related synucleinopathies[13], the landscape has never been more dynamic. From alpha-synuclein (α-syn) antibodies and LRRK2 inhibitors to repurposed GLP-1 receptor agonists and gene therapies, the therapeutic strategies are as diverse as the disease itself. What unites them is a growing reliance on biological markers to identify the right patients, confirm target engagement, and measure meaningful outcomes.
This article provides a comprehensive overview of the PD clinical trial ecosystem in 2026, with a focus on how blood-based biomarkers—and specifically alpha-synuclein seed amplification assays (SAA)—are enabling a new era of precision medicine in neurodegeneration.
The Biomarker Revolution: From Diagnosis to Trial Design
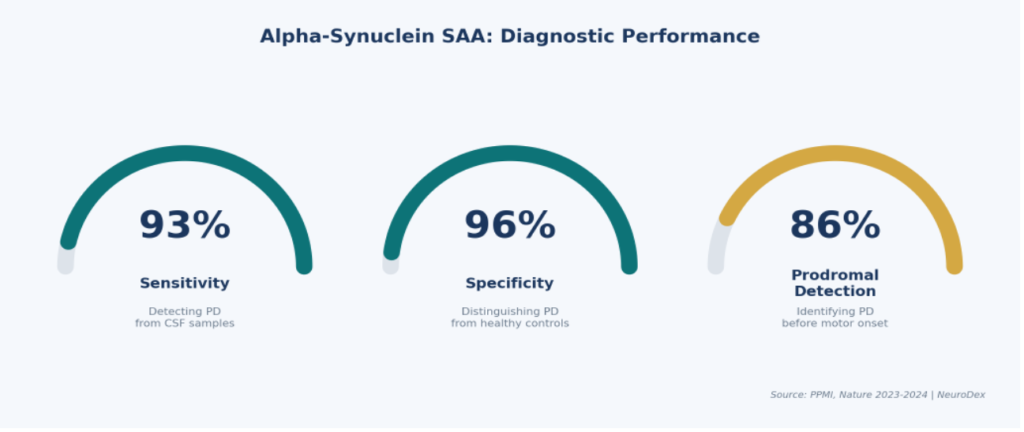
The single most transformative development in PD research over the past five years has been the validation of alpha-synuclein seed amplification assays (SAA). These assays detect misfolded α-synuclein aggregates—the pathological hallmark of PD—with remarkable precision. In the landmark Parkinson’s Progression Markers Initiative (PPMI) cohort of over 1,100 participants, SAA demonstrated 93% sensitivity and 96% specificity for distinguishing PD from healthy controls, including the ability to identify disease in prodromal stages before motor symptoms emerge[2].
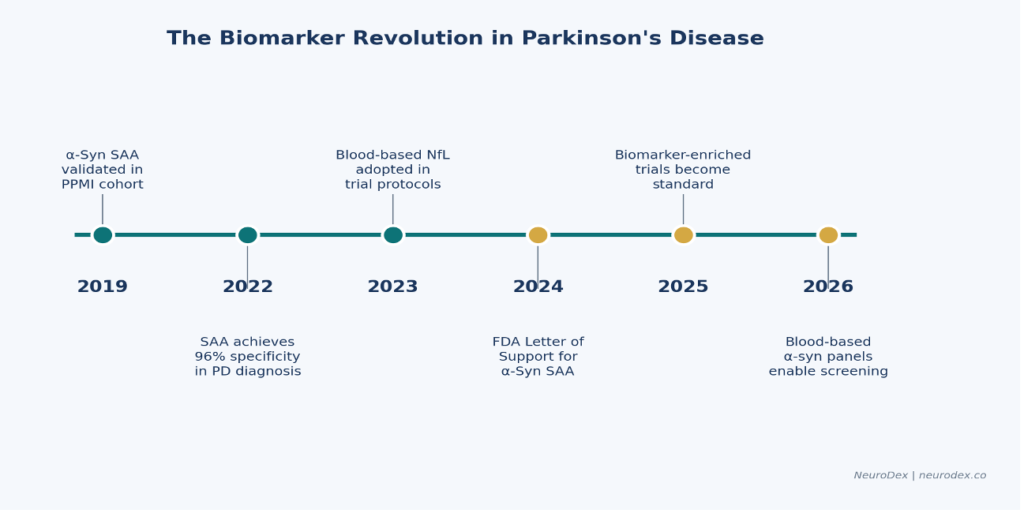
Figure 1: Key milestones in the PD biomarker revolution, from SAA validation to blood-based screening.
FDA Endorsement and Regulatory Momentum
In September 2024, the FDA issued a Letter of Support for alpha-synuclein SAA[3], formally recognizing its value for patient enrichment in clinical trials, establishing exploratory trial endpoints, and accelerating the development of PD therapies. The Critical Path Institute followed with published guidance recommending SAA for trial enrichment[4]—a landmark moment for biomarker-driven drug development.
This regulatory endorsement means that pharmaceutical companies can now use SAA-positive status as an enrollment criterion, ensuring that trial populations are biologically confirmed PD patients rather than relying solely on clinical diagnosis, which carries a known misdiagnosis rate of 15–25% in early disease stages.
Beyond CSF: The Promise of Blood-Based Biomarkers
While CSF-based SAA remains the gold standard, the field is rapidly advancing toward blood-based biomarker panelsthat can enable population-level screening[12]. Multiple biomarkers are emerging as complementary tools in the PD diagnostic and monitoring toolkit:
- Neurofilament light chain (NfL): A blood-based marker of neuronal damage increasingly incorporated into trial protocols for tracking disease progression and treatment response.
- Phosphorylated tau and amyloid markers: Critical for identifying co-pathology in PD patients, particularly those with Lewy body dementia overlap or Alzheimer’s comorbidity.
- Blood-based α-synuclein panels: Emerging assays from companies including NeuroDex are working to translate CSF-level sensitivity into accessible blood-based formats, enabling broader screening in clinical and research settings[15].
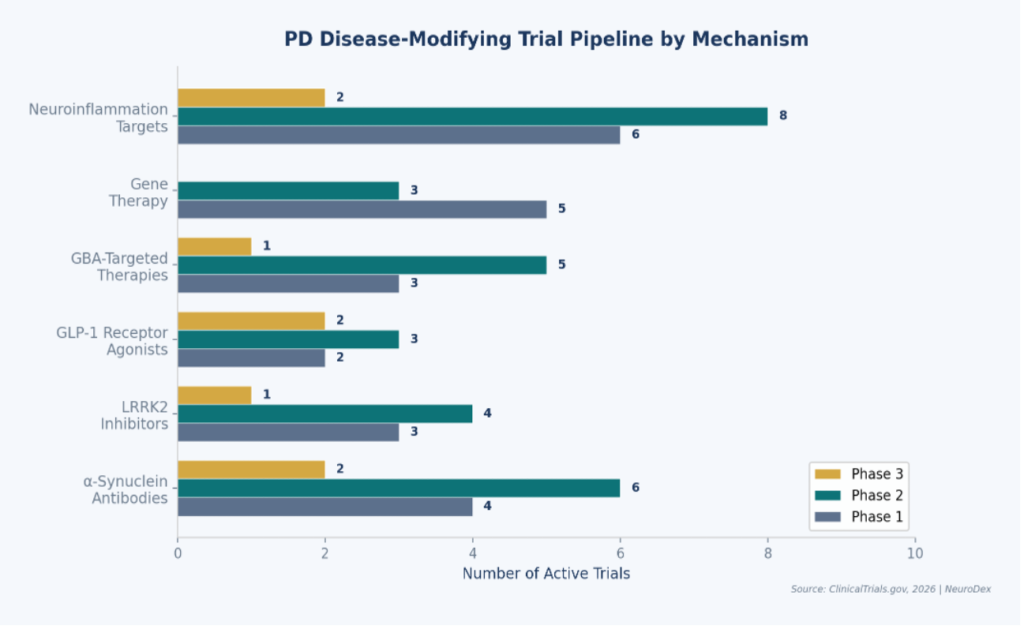
The 2026 Disease-Modifying Trial Pipeline
The PD clinical trial pipeline in 2026 is the most robust in history. Multiple therapeutic mechanisms are being pursued simultaneously, reflecting a growing understanding that PD is not a single disease but a spectrum of synucleinopathies with distinct genetic, molecular, and clinical subtypes[11].
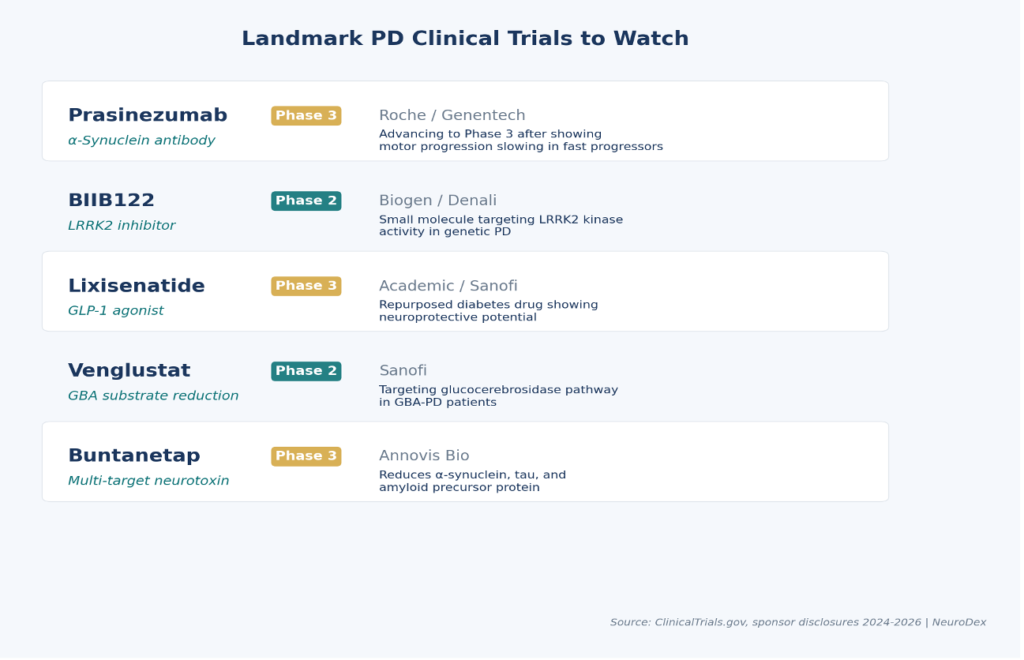
Alpha-Synuclein Antibodies: Prasinezumab Leads the Way
The most advanced α-synuclein-targeting therapy is prasinezumab (Roche/Genentech), an anti-α-synuclein monoclonal antibody now advancing to Phase 3. While the PASADENA Phase 2b trial initially missed its primary 12-month endpoint, extended follow-up revealed that early-start treatment groups showed meaningful slowing of motor progression over 2–4 years—particularly in patients identified as rapid progressors[5]. This finding underscores why biomarker-based patient stratification is essential: the therapeutic signal was strongest in a molecularly defined subgroup.
Roche announced in mid-2025 that prasinezumab would advance into Phase 3 studies[6], making it the first α-synuclein antibody to reach this stage. The decision to enrich enrollment with biomarker-confirmed rapid progressors reflects a broader industry shift toward precision trial design[14].
LRRK2 Inhibitors: Targeting Genetic PD
Mutations in the LRRK2 gene represent the most common genetic cause of PD, accounting for approximately 1–2% of all cases and up to 40% in certain populations. BIIB122 (Biogen/Denali Therapeutics) is a small-molecule LRRK2 kinase inhibitor that has demonstrated a favorable safety and tolerability profile in Phase 1/1b studies in both healthy volunteers and PD patients[7]. The program continues to evaluate optimal dosing and patient selection strategies, with genetic biomarker screening playing a central role in enrollment.
GLP-1 Receptor Agonists: A Surprising Second Act
Among the most exciting developments in PD therapeutics is the emergence of GLP-1 receptor agonists—drugs originally developed for type 2 diabetes—as potential neuroprotective agents. Lixisenatide and semaglutide are both under investigation in PD clinical trials, based on preclinical evidence of anti-inflammatory and neurotrophic effects[8]. Phase 3 studies are now underway, representing one of the most watched drug repurposing stories in neurology.
Gene Therapy and GBA-Targeted Approaches
Gene therapy trials targeting PD are expanding rapidly, with multiple AAV-based and CRISPR approaches under investigation. Simultaneously, therapies targeting the GBA (glucocerebrosidase) pathway—including venglustat (Sanofi) and ambroxol—aim to address the metabolic dysfunction that drives disease in GBA-PD patients, who represent approximately 7–10% of all PD cases[9].
Buntanetap (Annovis Bio) represents a novel multi-target approach, reducing production of α-synuclein, tau, and amyloid precursor protein simultaneously. Phase 3 studies are ongoing in both PD and Alzheimer’s disease.
Biomarker-Enriched Trial Design: The New Standard
The convergence of validated biomarkers and maturing therapeutic candidates is producing a fundamental shift in how PD clinical trials are designed. The era of enrolling broad, clinically diagnosed populations and hoping for a treatment signal is ending. In its place, a new paradigm of biomarker-enriched trial design is emerging.
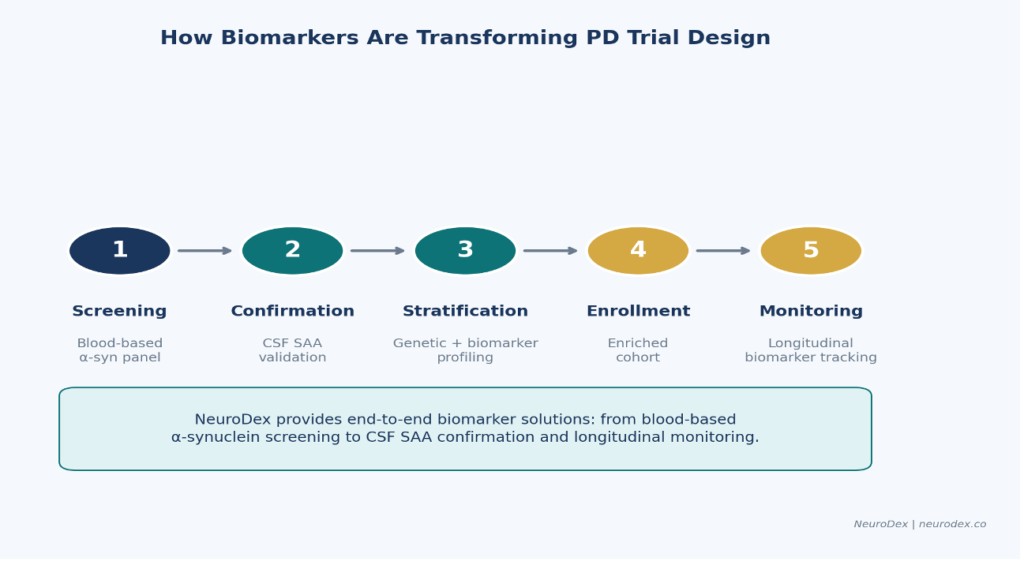
Figure 5: The biomarker-enriched trial design workflow, from blood-based screening through longitudinal monitoring.
This approach follows a structured workflow. First, blood-based screening using α-synuclein panels and NfL measurements identifies individuals likely to have synuclein pathology. Those who screen positive proceed to CSF SAA confirmation, providing biological certainty of disease. Genetic and biomarker profiling then stratifies patients by molecular subtype (LRRK2, GBA, idiopathic), ensuring the right patients receive the right therapy. Longitudinal biomarker monitoring throughout the trial provides objective measures of target engagement and disease modification—far more reliable than clinical rating scales alone.
The benefits are measurable. Biomarker-enriched trials can reduce required sample sizes by 30–50%, shorten trial timelines by eliminating misdiagnosed patients, and provide clearer efficacy signals that accelerate regulatory decisions.
NeuroDex: Enabling the Biomarker-Driven Trial Ecosystem
NeuroDex is positioned at the intersection of diagnostics, biomarker science, and clinical trial services. As the PD field transitions toward biomarker-enriched trial design, NeuroDex provides the tools and services that pharmaceutical companies, academic researchers, and clinical sites need to implement this new paradigm.
NeuroDex’s capabilities span the full biomarker value chain:
- Alpha-synuclein assay services: High-sensitivity α-synuclein detection for patient screening, diagnostic confirmation, and longitudinal monitoring.
- Clinical trial biomarker services: End-to-end biomarker solutions for trial sponsors, from protocol design and assay validation to sample processing and data analysis.
- Co-pathology assessment: Multi-analyte panels that identify co-occurring Alzheimer’s, tau, and amyloid pathology—essential for patient stratification in complex neurodegenerative disease trials.
- Research platform: A robust data and analytics platform supporting synucleinopathy research, enabling real-world evidence generation and biomarker discovery.
As disease-modifying therapies move toward Phase 3 and commercialization, the demand for reliable, scalable biomarker services will only intensify. NeuroDex’s infrastructure is designed to meet this demand—providing the diagnostic backbone that makes precision medicine in PD possible.
The Co-Pathology Challenge: Why Multi-Analyte Panels Matter
One of the most significant insights from recent biomarker research is that Parkinson’s disease rarely occurs in isolation. Studies from the PPMI cohort and other large registries have revealed that up to 50% of PD patients harbor co-occurring pathologies—amyloid plaques, tau tangles, TDP-43 inclusions, or cerebrovascular disease—alongside their primary α-synuclein pathology. This co-pathology burden has profound implications for clinical trials.
Patients with significant co-pathology may respond differently to α-synuclein-targeting therapies, confounding trial results and diluting treatment signals. Conversely, identifying patients with ‘pure’ synuclein pathology—or those with specific co-pathology profiles—enables more targeted enrollment and clearer efficacy signals. This is why multi-analyte biomarker panels that simultaneously measure α-synuclein, phosphorylated tau (p-tau 217, p-tau 181), amyloid beta 42/40 ratios, and neurofilament light chain are becoming essential tools for trial design[11].
NeuroDex’s co-pathology assessment services address this need directly, providing trial sponsors with multi-analyte profiling that enables precise patient stratification. Learn more about NeuroDex biomarker services.
A Global Perspective: Geographic Diversity in PD Trials
The PD clinical trial landscape is increasingly global. The United States remains the largest hub, hosting the majority of Phase 2 and Phase 3 studies, but Europe—particularly the United Kingdom, Germany, and France—has emerged as a strong contributor, especially for academic-sponsored biomarker studies. Asia-Pacific countries, led by Japan, South Korea, and China, are hosting an expanding share of trials, driven by large patient populations, growing regulatory infrastructure, and increasing pharmaceutical investment in the region.
This geographic expansion is critical for ensuring trial results are generalizable across diverse populations. Genetic risk factors for PD vary by ancestry—LRRK2 G2019S mutations are most common in Ashkenazi Jewish and North African Berber populations, while GBA variants show different frequency patterns across ethnicities. Biomarker-driven enrollment ensures that these genetic differences are captured and accounted for in trial design.
What Lies Ahead: The PD Trial Landscape in 2027 and Beyond
The next two years will be pivotal for Parkinson’s disease therapeutics. Prasinezumab Phase 3 results could deliver the first approved disease-modifying therapy for PD. GLP-1 agonist data will clarify whether metabolic pathways offer a viable neuroprotective target. LRRK2 and GBA programs will test the precision medicine hypothesis—can genetically defined subtypes yield better treatment responses?
Underlying all of these efforts, biomarkers will continue to mature. Blood-based α-synuclein assays are approaching clinical-grade performance, with the potential to transform PD screening from a specialist consultation into a routine blood test. Multiplexed panels combining α-synuclein, NfL, p-tau, and inflammatory markers will enable increasingly precise patient phenotyping.
For pharmaceutical companies planning PD trials, the message is clear: biomarker integration is no longer optional. Trials that incorporate biomarker-enriched enrollment, biological endpoints, and longitudinal monitoring will be more efficient, more informative, and more likely to succeed.
For clinicians and researchers, the expanding trial pipeline offers unprecedented opportunities to advance the science of PD while providing patients access to cutting-edge therapies. To explore active trials, visit ClinicalTrials.gov or the Michael J. Fox Foundation Trial Finder.
And for the millions of people living with Parkinson’s disease, the convergence of biomarker science and therapeutic innovation represents the most hopeful moment in the history of the disease.
References
- Dorsey, E.R., et al. (2018). “The Emerging Evidence of the Parkinson Pandemic.” Journal of Parkinson’s Disease, 8(s1), S3–S8. [Link]
- Siderowf, A., et al. (2023). “Assessment of heterogeneity among participants in the Parkinson’s Progression Markers Initiative cohort using α-synuclein seed amplification.” JAMA Neurology, 80(4), 407–417. [Link]
- U.S. Food and Drug Administration (2024). Letter of Support for Alpha-Synuclein Seed Amplification Assay. September 2024. [Link]
- Critical Path Institute (2024). Biomarker Qualification Opinion: α-Synuclein SAA for Clinical Trial Enrichment in Parkinson’s Disease. August 2024. [Link]
- Pagano, G., et al. (2024). “Prasinezumab slows motor progression in rapidly progressing early-stage Parkinson’s disease.” Nature Medicine. [Link]
- Roche Media Release (2025). “Roche advances prasinezumab into Phase III studies in Parkinson’s disease.” June 2025. [Link]
- Jennings, D., et al. (2023). “Safety and pharmacodynamics of BIIB122, a LRRK2 inhibitor, in patients with Parkinson’s disease.” Movement Disorders, 38(Suppl 1). [Link]
- Meissner, W.G., et al. (2024). “Trial of Lixisenatide in Early Parkinson’s Disease.” New England Journal of Medicine, 390(13), 1176–1185. [Link]
- Schneider, S.A. & Bhatt, M.H. (2025). “GBA-Associated Parkinson’s Disease: Pathogenesis and Therapeutic Strategies.” The Lancet Neurology. [Link]
- Michael J. Fox Foundation (2025). SAA Innovation Program: 2025 Request for Applications. [Link]
- Simuni, T., et al. (2024). “A biological definition of neuronal α-synuclein disease.” The Lancet Neurology, 23(7). [Link]
- Merchant, K.M., et al. (2024). “Blood-based biomarkers as enrollment criteria in Parkinson’s disease clinical trials.” Annals of Neurology. [Link]
- ClinicalTrials.gov (2026). Active interventional studies in Parkinson’s disease. Accessed April 2026. [Link]
- Garraway, L. (2025). “Precision Medicine in Neurodegeneration: The Roche Perspective.” Presented at AD/PD Conference 2025. [Link]
- NeuroDex (2026). Biomarker Services for Clinical Trials in Synucleinopathies. Company overview. [Link]
Further Reading & Resources
- Parkinson’s Progression Markers Initiative (PPMI) — The largest biomarker study in PD
- Michael J. Fox Foundation — Research funding and trial finder
- Critical Path Institute — PD Biomarkers Program — Biomarker qualification for trials
- gov — Parkinson’s Disease — Search active PD trials
- NeuroDex — Biomarker & Clinical Trial Services — Diagnostics, biomarkers, clinical trial solutions
About NeuroDex
NeuroDex provides diagnostics, biomarker services, and clinical trial solutions for Parkinson’s disease and synucleinopathies.
neurodex.co | info@neurodex.co

Leave a Reply