
Why NDE-Based Biomarkers Are Having a Moment
Let’s discover why NDE-based biomarkers are enabling earlier, more CNS-specific blood tests for Alzheimer’s, Parkinson’s, ALS, and other neurodegenerative diseases.
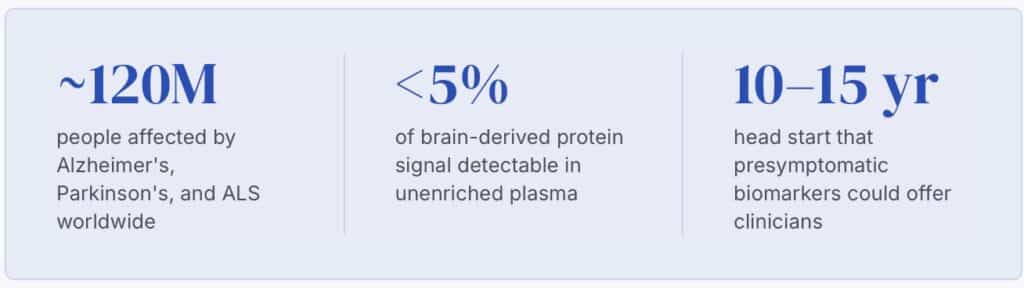
Neuron-derived extracellular vesicles (NDEs) have become the most closely watched approach in blood-based biomarker research for neurodegenerative disease. Here’s why NDE biomarkers are moving from academic labs into clinical trial design for Alzheimer’s, Parkinson’s, and ALS.
The Long Road to a Blood-Based Biomarker for Neurodegenerative Disease
For most of the history of neurodegenerative disease research, the biological evidence lived where the disease did—in the brain. Cerebrospinal fluid (CSF) biomarkers gave researchers access to a meaningful signal, but the barrier to collection was high: a lumbar puncture is invasive, not scalable, and poorly suited to the repeated sampling that disease monitoring demands.
Plasma-based biomarker testing seemed like the obvious fix. The problem was signal fidelity. The brain’s proteins are vastly diluted the moment they cross the blood-brain barrier, and peripheral noise—proteins from liver, muscle, and blood cells—drowns out what little central nervous system (CNS) signal makes it through. For years, blood-based biomarkers for neurodegeneration were considered technically interesting but clinically unreliable.
That is changing, rapidly, because of several simultaneous developments: ultrasensitive detection platforms, a better understanding of extracellular vesicle (EV) biology, and a shift in how regulators and drug developers think about biomarker-supported trial design. The FDA’s 2023 accelerated approval of lecanemab1 is one example of how diagnostic infrastructure is racing to keep pace with new therapeutics.
Five Trends Driving the Shift to Blood-Based Neurodegenerative Biomarkers
01 Ultrasensitive detection has arrived
Single-molecule array (Simoa) technology and related platforms pushed the lower limit of detection for proteins like neurofilament light (NF-L) and GFAP into the femtomolar range.2 Proteins that once required CSF to measure reliably can now be quantified from a standard blood draw. The technical floor that made plasma biomarkers impractical has largely been cleared.
02 Regulatory momentum behind blood-based diagnostics
The FDA’s accelerated approval of lecanemab in 2023—tied explicitly to amyloid burden—created a new downstream demand: fast, accessible patient stratification. CSF and PET imaging can confirm amyloid status, but neither is scalable to the primary care setting. Blood-based p-tau217 and Aβ42/40 ratios are now seen as the practical bridge between a patient’s first concern and a specialist’s diagnostic workup.3 Regulatory pathways are following that clinical reality.
03 Drug development needs better trial design tools
Failed trials in neurodegeneration have frequently been attributed to patient heterogeneity—enrolling participants who were too advanced, or whose biology didn’t match the mechanism being targeted. Biomarkers that stratify, stage, and monitor disease state in real time are now recognized as essential infrastructure for clinical development, not a downstream add-on. Sponsors are investing accordingly.
04 Extracellular vesicle biology has matured
EVs were once dismissed as cellular debris. Over the past decade, the field has established them as structured intercellular communication vehicles carrying proteins, nucleic acids, and lipids that reflect the biology of their cell of origin.4Critically, EVs that originate in neurons cross the blood-brain barrier intact—and their cargo, protected from proteolytic degradation in circulation, preserves biomarker signal that free plasma protein does not.
05 Presymptomatic detection is the new standard of ambition
The disease model in neurodegeneration has shifted. Alzheimer’s and Parkinson’s are now understood to develop over decades before motor or cognitive symptoms appear.5 If biomarkers can detect pathological change 10–15 years before symptom onset—and accumulating evidence suggests they can—the intervention window that opens is transformative. This has changed the research question from “can we diagnose faster?” to “can we intervene before damage is done?”
What Makes NDE Biomarkers Different From Standard Plasma Biomarkers
General EV populations in plasma reflect contributions from every cell type in the body. For CNS biomarker applications, that’s a problem: the neuron-derived signal is present, but it’s embedded in a background of EVs from platelets, endothelial cells, red blood cells, and more. Measuring TDP-43, tau, or synaptic proteins from an unenriched EV fraction is like listening for a single instrument in a crowd.
Neuron-derived EVs carry cargo that is biologically specific, structurally protected, and analytically accessible in ways that free plasma proteins simply are not
Isolation of neuron-derived extracellular vesicles (NDEs)—typically using surface markers like L1CAM, NCAM, or EPCAM variants enriched on neuronal membranes—allows researchers to pull down a CNS-specific fraction from a standard blood draw. NeuroDex’s ExoSORT™ platform was built specifically to standardize this NDE isolation step. Once enriched, the NDE cargo tells a detailed story: which proteins are misfolded, which pathways are dysregulated, which cells are under stress.
The NDE approach makes several previously difficult measurements tractable. TDP-43 pathology, central to ALS and a subset of frontotemporal dementia, has been notoriously difficult to track with peripheral biomarkers—but TDP-43 is well-represented in NDE cargo.6 Synaptic markers like synaptotagmin and SNAP-25, which require CNS specificity to be interpretable, become measurable with confidence when the EV fraction is neuronally enriched. Proteins like NRF2 and NFkB that reflect neuroinflammatory state similarly emerge from the noise once the non-CNS background is removed.
ALS has historically lacked validated peripheral biomarkers tied to disease mechanism rather than just neuronal loss. NDE-derived TDP-43 and synaptic protein profiles offer a window into the biology of affected motor neurons—potentially enabling the kind of disease staging and treatment response monitoring that clinical trials in ALS urgently need.
This is not theoretical. A growing body of published literature demonstrates that NDE cargo profiles differ between patients with neurodegenerative disease and healthy controls, and in some cases track with disease progression. The field is moving from proof-of-concept to analytical validation, and from academic labs toward clinical-grade workflows.
The Future of NDE Biomarker Validation and Clinical Adoption
The next challenge is standardization. EV isolation methodology varies substantially across laboratories: centrifugation protocols, immunocapture conditions, antibody lots, and storage conditions all affect yield and cargo composition. For NDE-based biomarkers to move from research tool to clinical infrastructure, the field needs reproducible, validated workflows that hold up across sites, operators, and time.
This is where the opportunity is largest—and where the gap between current practice and clinical readiness remains widest. Researchers who want to use NDE cargo as outcome measures in trials, or as patient stratification tools, need platforms they can trust to deliver consistent results. That means analytical sensitivity sufficient to detect disease-relevant signal at low NDE concentrations, specificity confirmed against non-neuronal EV populations, and documented performance across sample types and handling conditions.
The momentum is real. Investment in blood-based neurodegenerative diagnostics has accelerated meaningfully since 2022, and academic–industry collaborations around EV-based biomarkers are growing. The regulatory environment is more receptive to biomarker-supported endpoints than it was five years ago. And the clinical unmet need—faster, less invasive, earlier diagnosis—has never been more widely acknowledged.
NDE-based biomarkers are not the only approach to blood-based CNS diagnostics. But they offer something the alternatives do not: biological specificity at the source. The signal comes from neurons, reflects neuron biology, and survives the transit from brain to blood in a protected, measurable form. For diseases defined by what happens to neurons, that specificity matters.
The moment is here. The infrastructure to take advantage of it is what the field is now building.
Sources
- U.S. Food and Drug Administration. “FDA’s Decision to Approve New Treatment for Alzheimer’s Disease.” 2023. fda.gov
- Rissin, D. M., et al. “Single-molecule enzyme-linked immunosorbent assay detects serum proteins at subfemtomolar concentrations.” Nature Biotechnology, 2010. PubMed
- Janelidze, S., et al. “Plasma P-tau217 in Alzheimer’s disease: relationship to other biomarkers, differential diagnosis, neuropathology and longitudinal progression to Alzheimer’s dementia.” Nature Medicine, 2020. PubMed
- Théry, C., Witwer, K. W., et al. “Minimal information for studies of extracellular vesicles 2018 (MISEV2018).” Journal of Extracellular Vesicles, 2018. PubMed
- Jack, C. R., et al. “NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease.” Alzheimer’s & Dementia, 2018. PubMed
- Sproviero, D., et al. “Pathological proteins are transported by extracellular vesicles of sporadic amyotrophic lateral sclerosis patients.” Frontiers in Neuroscience, 2018. PubMed

Leave a Reply